


 July 16, 2012
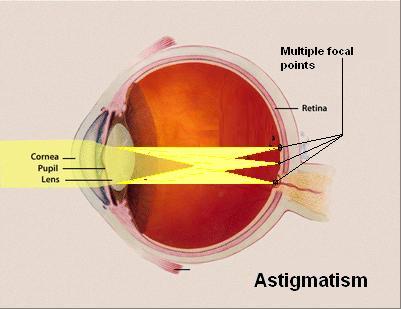
July 16, 2012 Astigmatism is a condition in which the light rays do not refract equally in all meridians of the eye. For the purpose of division, two imaginary meridians of the eye are defined, perpendicular to each other. The term astigmatism is of Greek origin and it literally means “no point”.
At spherical lens, where all the meridians have the same curvature, light rays can be directed (focused) into one point. Astigmatic lens, due to unequal curvature of meridians, cannot create image of an object in one point. Instead of one focal point, astigmatic system creates two focal lines separated by a focal interval. Length of the focal interval is a measure of a degree of astigmatism, and correcting this fallacy can only be done by merging two focuses into one.

Causes:
Astigmatism can be an error of curvature, directing light into the center, or light refraction index.
Astigmatism of curvature is mostly found in the cornea. The anomaly is usually inherent, but it occurs in a small degree almost at every person. The most common error is the one at which the vertical curvature of the cornea is larger than the horizontal one. This condition is called direct astigmatism and it is concerned as normal, physiological. It probably occurs because of the constant pressure of the upper eyelid on the eye. Studies show that at birth the cornea is almost perfectly spherical. Later, in childhood at the age of 4, in 65 % of children astigmatism can be found, and at the age of 7 in 95 % of children. This is a proof that direct (“normal”) astigmatism increases with time, but during aging it disappears or becomes inverse (“reverse”) astigmatism at which the vertical curvature is smaller than horizontal.
Acquired astigmatism is a rare phenomenon. Corneal disease can cause this error. An extreme example of this is keratoconus, and corneal inflammation and ulceration have the same effect. Trauma of the cornea can also cause astigmatism; in this category especially important is the surgical trauma, usually due to lens surgery. Corneal astigmatism can occur due to swelling of eyelids caused by harmless halacion or tumor. Transient astigmatism can be induced by pressing the cornea with a finger, by contracting the eyelids or by the effects of the external eye muscles.
Astigmatism of curvature can also exist in the lens. In most cases there are only small anomalies, but sometimes, like when it comes to lentikonus – lens in the shape of a cone, there is a significant astigmatism. Often is the lens set aslant, or it is out of line of optical system because of what a disorder of directing light into the center line and astigmatism occur. Finally, a small number of astigmatism of refractive index occurs naturally in the lens. Usually this is a small shift from the normal refractive index, but sometimes it is a cause of a significant disorder.
Types of astigmatism:
Astigmatism at which the two main meridians form the right angle is liable to correction and it is called regular astigmatism. In most cases, meridians of the greatest and the smallest curvature are nearly or completely horizontal or vertical. If the meridians of the greatest and the smallest curvature form a right angle, but are not vertical or horizontal, that kind of regular astigmatism is called oblique astigmatism. When axes are not at a right angle, but they obliquely intersect, the optical system can still be repaired with sphero-cylindrical combination, and the condition can be called double-oblique astigmatism. When irregularities of meridians’ curvature cannot be related to any geometric figure, the condition is called irregular astigmatism.
Regular astigmatism
Regular astigmatism is classified into:
- Simple astigmatism is the one at which one of the focuses falls on the retina. The other focus falls in front of the retina or behind it, which means that one of the meridians is myopic or hyperopic. Depending on the location of the other focus, we distinguish between simple myopic and simple hyperopic astigmatism.
- Complex astigmatism is the one at which none of the focuses falls onto the retina, but they are both in front of it and behind it. The condition of refraction is then completely myopic or hyperopic: complex myopic and complex hyperopic astigmatism.
- Mixed astigmatism is the one at which one focus is in front of the retina, and the other one is behind it, therefore is the refraction in one meridian hyperopic, and in the other one it is myopic.
The usual physiological type of astigmatism at which the vertical curvature is larger than the horizontal is called direct astigmatism; in the opposite case it is called indirect astigmatism.
Irregular astigmatism
At irregular astigmatism curvature in different meridians is very irregular. A small degree of this fallacy usually develops because of the lens structure, but it is so small that it is considered insignificant. This irregularity of the lens sometimes increases due to illness. A significant degree of irregular astigmatism often is found only in corneal disease, usually due to improper healing of injury, inflammation or ulceration. In this case, visual fallacy caused by astigmatism is reinforced by the presence of corneal turbidity, and any attempt at correction is often difficult or even impossible. Conical cornea (keratoconus), which is convex outwards in the form of a cone, is often visible. The eye becomes myopic and astigmatic. Correction of vision, in this case, is difficult due to disease progression and constant changes of optical condition.
Treatment of irregular astigmatism is often unsatisfactory. Correction of vision with glasses is often quite insignificant, but in some cases it is quite satisfactory. When it comes to keratoconus and other cases of turbidity, contact lenses are known to help. When neither eyeglasses nor contact lenses help, surgery should be given a try.
Symptoms:
With astigmatism of a significant degree, the eye cannot create a clear image on the retina and visual acuity is significantly reduced. In order to create a clear image the patient is trying to focus onto the retina one of the focal lines – the meridian which is closer to directing light onto the retina. If both meridians are approximately at the same distance, the vertical focal line is generally taken. This is a natural process of adjustment because most objects, usually capital letters, are impossible to figure out if they are vertically deformed. Because of directing attention to the focal line, astigmatic person sees the environment in a peculiar way. Circles elongate into ovals, the point of light looks elongated. If astigmatic person observes two vertical lines, one of them will be blurred. In any case of regular astigmatism one line will be clear, while the other one will be blurred. This is used to diagnose astigmatism using certain geometric figures. If the cylinder axis is aslant, the head is often tilted to one side to reduce deformation of the image. This habit can lead to development of scoliosis, among children. In all cases there is a tendency of closing eyelids at half, as with myopia, because that way rays from one meridian are cut, and so the object of observation can become clearer.
Constant effort during attempts of accommodation (adjustment) in order to create a clear image causes symptoms of weakness and eye strain. This is particularly true in cases of small astigmatic fallacies where accommodation success is good, so the eye is stimulated to a greater effort. In most cases small fallacies do not cause discomfort, and they are accepted as natural. In other cases, the existence of a series of symptoms is possible – headaches that vary from mild frontal pain to severe explosive headache, and a variety of disorders such as, dizziness, irritability, fatigue. The most difficult symptoms are visible at hyperopic astigmatism in which accommodation is especially emphasized. Unlike a myopic person, an astigmatic squints while looking at close range and at a distance. As myopic people, astigmatic ones hold the text close to their eyes while reading.
The most common symptom of astigmatism is blurred vision. With mild errors, the person does not even have to notice the existence of the disorder. A higher degree of astigmatism can cause significant vision problems. Children with a higher degree of astigmatism usually do not know that they have blurred vision because they have never seen a focused, clear image of an object.
Some of additional symptoms of astigmatism:
– Blurred vision while trying to read small letters
– Difficulty in reading
– Diplopia
– The appearance of nonexistent images
– The impossibility of seeing close or distant objects without squinting
– Children may have problems with concentrating on printed words and straight lines; they may have headaches and complain about eye strain
Treatment:
If they do not reduce visual acuity and do not cause visual impairment and eye fatigue, small fallacies do not require treatment. If some of these symptoms are present, it is necessary to pay close attention to astigmatism. Correcting the fallacy is very important because the patient tries to correct every residual departure from normal focus with efforts of the eye, and therefore, the symptoms may continue or even worsen. Cylindrical defect is tried to be corrected completely. Sometimes, at adults who have never worn eyeglasses or contact lenses, unexpected effect of cylinder may result in impaired image of an object. In such cases, cylinder therapy of lower intensity can be started, with gradual approaching to required strength.
Except with glasses, astigmatism is also corrected with appropriate lenses. When the total astigmatism is exclusively a consequence of corneal surface disorder, and if the refractive properties of lens materials, tears, and cornea are the same, then properly positioned lenses can correct the fallacy completely. Since these refractive properties are not completely equal, nor is the astigmatism always caused by corneal disorder, so even after positioning contact lenses there is always a certain degree of astigmatism. This residual astigmatism appears due to the real residual astigmatism which mostly occurs due to ocular lens and the properties of contact lenses. Residual astigmatism is very difficult to predict with diagnostic tests; luckily, it is usually very small and it has very small effect on visual acuity, so it can be disregarded.
Contact lenses can correct astigmatism of the cornea and the lens. There are a number of contact lenses, and for their choice it is best to consult with a medical specialist of ophthalmology. A procedure, called orthokeratology or Ortho-K, also uses contact lenses – rigid lenses are worn several hours daily until the curvature of the eye is partially corrected. Afterwards, the lenses are worn more seldom to maintain the new shape of the eye. If the treatment is completely stopped, the eye returns to its original form. Alternative to contact lenses are eyeglasses. Surgical branch which treats astigmatism is called refractive surgery because it corrects disorders of light refraction. Its purpose is to reshape parts of the eye. The methods are:
– LASIK surgery (LASIK = Laser-assisted in situ keratomileusis) is a procedure at which the doctor uses an instrument, keratocysts, with which a thin, circular incision on the corneal surface is made. The created lobe is lifted and afterwards with excimer laser the cornea underneath the lobe is reshaped. Excimer laser is different from other lasers because it does not produce heat.
– Photorefractive keratectomy (PRK) – application of high-energy ultraviolet light (wavelength 193 nm) that is generated from the argon-fluoride excimer laser, and it is applied to the surface of the cornea in order to change its shape and correct refractive fallacies. The physical process of shaping the cornea in this manner is called photoablation. This surgical procedure reshapes the center of the cornea which needs to be slightly flattened at myopic people, or bulged at hyperopic people.