


 July 16, 2012
July 16, 2012 Keratitis is the inflammation of the cornea of the eye. There is difference between superficial keratitis which involves the superficial layers of the cornea and usually does not leave a scar; and deep keratitis which involves deeper layers of the cornea and usually leaves a scar which impairs vision if it is near the visual axis.
Causes:
Causes of keratitis may be multiple conditions and diseases of the whole body which can affect cornea (e.g. bacteria, viruses, fungi, neuro-paralitic keratitis at paralysis of the first branch of n. trigeminus), as well as unknown causes in some cases (e.g. sclerosis keratitis, Ulcus rodens).
Pathogens:
Acanthamoeba keratitis – severe inflammation of the cornea caused by amoebas (mostly Acanthamoeba) which ususally appears at contact lens wearers.
Bacterial keratitis – inflammation that mostly occurs after injuring the cornea, as a complication of conjunctivitis, as a result of decreased immunity or wearing contact lenses. The most common infective agent is Staphylococcus aureus, or at contact lenses wearers Pseudomonas aeruginosa.
Viral keratitis – caused by viruses, mostly Herpex simplex viruses.
Symptoms:
Symptoms at the beginning are very similar to those of conjunctivitis: light sensitivity of the eye, photophobia, redness of the conjunctiva and the feeling of discomfort in the eye; which might eventually turn into severe pain, loss of vision and pus formation.
Types of keratitis:
Keratitis herpetica
The cause of this disease is Herpes Simplex virus. Viral types of keratitis are more common than bacterial ones. The disease begins suddenly, unilaterally with the occurrence of pain and the feeling of an alien object in the eye. It mostly appears at middle-aged men, sometimes connected with a trauma. Keratitis herpetica is mostly a secondary manifestation of infection which appears after the cold, pneumonia or the flu.
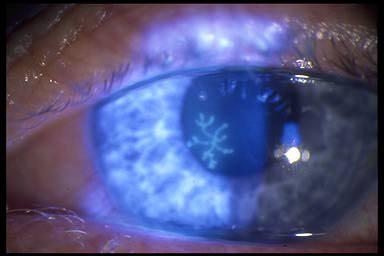
Keratitis herpetica superficialis
There are small, grey, star-like bleariness appearing on the epithelium of the cornea, from which emerge bubbles which burst and leave shallow defects of epithelium. The disease has a chronic flow. The complications are: iridocyclitis, glaucoma, keratitis metaherpetica.
Symptoms: photophobia, epiphora (overflow of the tears), feeling of an alien object in the eye, blepharospasm, neuralgic pain, decline of vision.
Treatment: removal of infiltrated tissue by showering, antibiotic ointment, atropine, scopolamine, virostatics, acyclovir, interferon.
Keratitis herpetica parenchimatosa
The cause of herpes enters the parenchyma through the Bowman membrane. Its occurrence is attributed to immunologic reactions (viral allergy), and not to direct effect of herpes viral infection. It leads to disciform blur of cornea, loss of gloss and smoothness.
Symptoms: photophobia, epiphora, pain, decline of vision, decreased sensibility of cornea. The complications are: ulcer, secondary infection, recidives.
Treatment: cortisone preparations (this is the only type of herpetic keratitis at which corticosteroids can be used).
Bacterial keratitis (ulcus serpes corneae)
Ulcerous keratitis or ulcer of the cornea. A disease that occurs by exogenous infection of the surface of the cornea, and then spreads into the depth. The causes are streoptococcus or pneumococcus. The precondition for infection is the damaging of corneal epithelium, because the epithelium of healthy cornea is resistant to penetration of the causal agent into the depth.
The cause of infection may be:
a) chronic infection of lacrymiform
b) conjunctival contagious furrow
The disease occurs at people who are often exposed to damaging the cornea, as are stonecutters, forestry workers…
Symptoms: infiltration around the injured part on the cornea, the bottom of ulcer is blurred, grey and lifted, hyperemia of the iris, blurriness of aqueous humor, accumulation of pus in the bottom of the anterior chamber, photophobia, epiphora, blepharospasm, chemosis of the conjunctiva, feeling an alien object in the eye, pain.
Treatment: Sulphonamids and antibiotics in form of eye drops and ointments, midriatics, showering with iodine tincture. Results of bacterial keratitis are irregular astigmatism and decline of vision.
Keratomycosis
The primary infection appears after small injuries of the cornea. The secondary infection appears at primary bacterial and viral infections, because the antibiotics that were treating the primary disease opened the way to fungi. Fungal eye diseases on cornea appear mostly as central ulcer.
The causes are Aspergilus, Candida albicans, aktinomicosis.
Symptoms: strictly bordered ulcer with grey-yellow edge, yellow-white infiltrate in shape of a plate, dry surface that looks like chalk, hypopion, photophobia, epiphora, severe pain that is not appropriate to given results.
Treatment: showering the ulcer with iodine tincture, antimicotic preparations (Amphotericin).
Keratitis parenchymatosa (allergic keratitis)
Deep bilateral inflammation of cornea which is encountered at lues as congenital form. It occurs between the ages of 5 and 7, and then in puberty, mostly at girls.
Cause: Changes in corneal parenchyma are a result of allergic-hyperergic reactions.
Symptoms: edema of endothelium, cloud-like blurriness in deep layers of cornea, cornea gets stabbed look, growing of blood vessels into the cornea, after 6 to 8 weeks blurriness wearies off but blood vessels in the cornea obliterate and remain as soft shadows, pain, epiphora, photophobia, blepharospasm.
Except pathologic changes on eyes, at lues occurs saddle-like nose, expressed frontal bone, scars on the skin around the corners of lips, hearing decline, Hutchinson’ teeth, inflammation of joints.
Treatment: parenteral penicillin, local cortisone therapy.
Actinic keratitis
Actinic keratitis is a painful eye condition caused by the exposure to ultraviolet rays as in welding arc (“welding eye”), solarium light, reflection of sunlight from the snow (“snow blindness”), greater surfaces of water (“swimmer keratitis”), sand (“desert blindness”), electric explosion etc. Intensive ultraviolet rays that the eye has absorbed cause superficial, but very painful and uncomfortable keratitis.
Symptoms:
Symptoms mostly occur several hours after the exposure and typically, they spontaneously withdraw within 36 hours. The feeling is described as if having sand in eyes, discomfort and pain. The symptoms are excessive lacrimation, blepharospasm, photophobia; fluorescein color will detect superficial damages of cornea under the blue light, narrowed pupils (in some cases this symptom can last from 96 to 128 hours).
Treatment:
Examination of cornea – search for an alien body, if the patient is fine with bandaging, the bandage is to be placed on the eye with stronger symptoms; prescribe a painkiller; topical (local) antibiotics in the form of eye drops or ointments, due to preventing infection; cold dry compress
Punctiform keratitis
It is marked by multiple tiny defects of cornea epithelium. It is usually conjoined with conjunctivitis.
Causes:
It is mostly caused by adenoviruses. Other causes are contact lenses, ultraviolet rays (welding without mask), and dry eye (keratoconjununctivitis sicca).
Treatment:
Topic antibiotics should be used due to prevention of bacterial super-infection. After curing the dry eye fake tears should be used all the time (s. the syndrome of dry eye).
Oftalmic herpes zoster
Zoster keratitis is a result of infection of trigeminal ganglion with varicella virus (Varicella zoster virus). It usually occurs at older people and those with low immunity.
Symptoms: pain and soon occurrence of vesicles in areas of ophthalmic nerve branching (eye, eyelids, forehead, nose, upper part of the face). Vesicles burst and turn to scabs which sometimes leave scars – as with varicellas. On cornea may appear punctiform keratitis or ulcer, followed by conjunctivitis.
Treatment: Antiviral drugs, topically and per os. Since the pain in first couple of weeks is severe, painkillers should also be taken.
Fungi keratitis
Usually appears after injuries in farming or gardening, and lately, even after extended wearing of contact lenses. It is characterized by obstinate ulcer, often covered with white deposits.
Treatment: Antimicotics topically; in the most severe cases even systemic.